

It is a condition resulting from disruption of blood supply to the part of femoral head, leading to death of affected part and collapse of overlying cartilage. It is also known as Osteonecrosis.
Common causes of Osteonecrosis are Injury like Neck of femur fracture or hip dislocation, excessive consumption of alcohol, long term steroid intake, abnormalities of blood such as sickle cell disease etc. Many times it is idiopathic (without recognizable cause) and it is bilateral in up to 80% of cases.
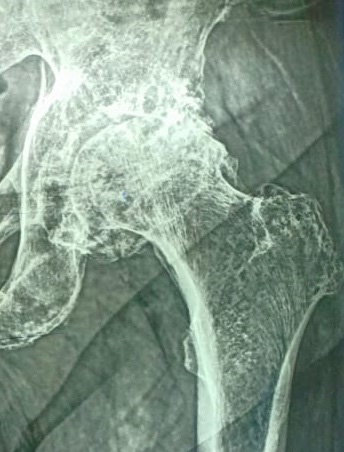
Patients of AVN complain of groin and thigh pain, often radiating to knee; restriction of movement of hip joint and limp. Most of the time onsets of symptoms are insidious. X ray of Hip joint may be normal in early stage and diagnosis can be made on MRI.
Most of the patients present with advance stage of AVN, when medical management is not possible. Surgical procedure known as Core Decompression is possible if femoral head is not collapsed. In this procedure multiple drilling is made in to affected area of head under image intensifier guidance. This is minimally invasive procedure. This can be combined with stem cell insertion or bone grafting.
In advance stages (after head is collapsed) Total Hip replacement is the only definitive treatment. Cementless THR with Ceramic-on-ceramic articulation gives good function and long term survival of implant.
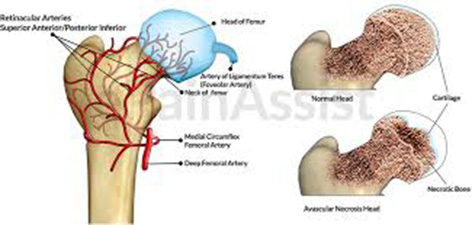 Avascular Necrosis (AVN)
Avascular Necrosis (AVN)
Osteoarthritis occurs due to degeneration (Wear and tear) of hip joint cartilage. Incidence of Osteoarthritis of hip is less in India as compared to western world. Common causes are Old age, fractures around hip joint, obesity or overuse. Conservative treatment includes weight loss, physiotherapy, use of cane and pain medications. Total Hip replacement is required if pain is disabling and interfere with activity of daily living.
It is a form of inflammatory arthritis primarily affecting spine. Symptoms usually start in early adulthood and characterized by episodes of pain and stiffness of back. Hip, shoulder and small joints of Hands and feet are also affected. Involvement of hip is often bilateral and is associated with stiffness. In advance stages hip may be completely fused. Disease is often hereditary. Patients may have gene that produce a protein called HLA B 27. Disease can be treated by medication in early stages in consultation with Rheumatologist. Physiotherapy helps to prevent ankylosis (Bony fusion). Advance stages require Total hip Replacement.
Rheumatoid arthritis is a form of inflammatory arthritis where body's immune system attacks the joints. It is characterized by multiple joint pain, usually bilateral and symmetrical. Hands, feet, knees and hips are affected by Rheumatoid arthritis. Diagnosis can be made with help of X ray and laboratory investigations. Hip pathology is associated with osteoporosis and deformity of joint, making ambulation difficult and painful for patients. Total hip replacement is challenging yet satisfactory treatment option for these patients.
Total hip replacement is one of the options for treatment of fracture Neck of femur in elderly patients. It is also required when internal fixation fails or patients develop painful arthritis after femoral or acetabular (Socket) fracture.
Here femoral stem and acetabular cup are fixed to the bone using bone cement. This type of prosthesis is preferred in elderly patients with osteoporosis.
Cementless prosthesis have special coating on its surface, which provides initial stability and facilitates bone growth to provide durability. Both femoral and acetabular components are inserted without cement. It is preferred in younger patients with good bone quality.
Here one component is cemented and other is cementless. Mostly it is the femoral stem that is fixed using cement.
Here Metal femoral head articulates with ultra high molecular weight poluethylene (UHMWPE) acetabular liner. It is the oldest and widely used articulation. This articulation carries risk of wear of plastic and osteolysis in long term.
Here Ceramic femoral head articulates wit h UHMWPE acetabular liner. Wear rate of this articulation is less compared to Metal-on-poly.
Here femoral head as well as acetabular liner are made up of ceramic. It has least wear among all articulation and is preferred in young active population.
Dual Mobility cups have two point of articulation – one between acetabular shell and polyethylene and other between Polyethylene and metal/ceramic head. It is preferred in patients with higher risk of instability.
 Ceramic-on-ceramic
Ceramic-on-ceramic
 Ceramic-on-poly
Ceramic-on-poly
 OA Hip
OA Hip
 After THR
After THR