

Revision TKR is required when primary TKR fails for some reason. It is more complex procedure and requires special implants.
Total knee replacement survives for more than 15 years in 90% of the cases. In few patients prosthesis becomes loose due to weakening bones. These patients complain of pain, swelling and difficulty in walking. Diagnosis can be made on X ray or CT scan. They require Revision TKR surgery. If only one component is found loose, we can revise only one component.
Early instability result from improper ligament balancing at the time of Primary TKR. Late instability can be due to wear of articular plastic. This can be revised using semi-constrained or Hinge prosthesis.
Infection around Knee prosthesis may require to take out the prosthesis, debride thoroughly and insert Antibiotic loaded cement spacer . This is followed by 4 to 6 weeks of IV antibiotics. Once infection is cured, second surgery is required to remove the spacer and put a new prosthesis. This is called Two stage revision surgery.
Fracture around TKR can be fixed using plate and screw if implants are stable. If implants are loose, revision TKR will be required. Diagnosis can be made on X ray or CT scan.
Most of the patients are pain free with in 3 months of Primary TKR, but up to 10% patients complain of some sort of pain for longer period. This may be due to errors in alignment, tissue irritation, metal allergy or neuropathy. These patients require through investigation and revision surgery is offered if rectifiable cause is found.
This type of implant is used when ligaments are lax and revision is required to treat instability.
Hinge prosthesis is required when there is complete absence of ligament. It is also required in Re-revision surgery or in cases of extensive bone loss.
This is required when there is bone loss in distal femur or proximal tibia. It provides stability to revision prosthesis.
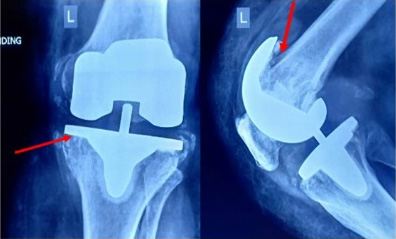 Before (Prosthesis loosening)
Before (Prosthesis loosening) After Revision TKR
After Revision TKR